


Gordon Grover is the founder of Specialized Property Consulting (SPC), a client-side project management firm specializing in complex health and laboratory projects. Based in Toowoomba, with the firm's largest office in Brisbane, he has spent close to twenty years delivering hospitals, laboratories, and other highly technical facilities for government and institutional clients.
In this interview, Doug Vincent (Co-founder and CEO of Mastt) asks Gordon why these projects demand specialists, how his team manages risk from feasibility through to commissioning, and where he thinks the industry has gone backward on design and delivery.
Why Hospital and Laboratory Projects Are a Specialist PM Skill
Plenty of project managers can run a fit-out or an office build, but healthcare construction is a different discipline. Far fewer can deliver a working hospital. Gordon explains what separates the two and why experience is the entry ticket.
Q: Client-side PMs deliver all kinds of projects. What makes complex health and laboratory work a specialist skill set?
A: Client-side project management is all about risk management, whether that's risk to your program, your budget, the quality of the build, or the quality of the design. You can't manage risks if you don't know what they are, and the best way to know what they are and how to manage them is to have done it before.
You can't walk in the door and learn that off the cuff.
Spaces like PC3 (Physical Containment Level 3) and PC4 (Physical Containment Level 4) labs, intensive care units, and theaters are highly technical and complex. You can't drag experience across from a fit-out or an industrial project and expect to know what's coming.
You build that knowledge by working for a business, and alongside people who have delivered these projects before.
“Client-side project management is all about risk management, and you can't manage those risks if you don't know what they are. The best way of knowing them is by having done it before.”
- Gordon Grover, Founder and Managing Director of SPC
Q: Across health, aged care, and laboratories, which spaces are the most complex to deliver?
A: Health is the most complex, with laboratories close behind. Within health, the standouts are CSSDs (Central Sterile Services Department) and ICUs (Intensive Care Units).
A CSSD is the central sterilizing unit, where all the theater instruments go to be cleaned. They're full of equipment such as sterilizers, washers, and dryers, all integrated and monitored, with high infection-control requirements throughout.
A general hospital only has one, so when you refurbish a CSSD, you have to keep it running, or the whole hospital shuts down. Pulling out old sterilizers and replacing them while keeping everything operational usually means a ten- or fifteen-stage project with a heap of controls along the way.
Intensive care units and theaters are similarly complex because of the equipment integration. If a pendant or a piece of equipment fails during an operation, it can be life or death.
How to Manage Risk on Hospital Construction Projects
Client-side delivery on health projects lives or dies on risk. Gordon walks through when to engage, how risks get surfaced, and the ones that recur in every live hospital.

Q: When should a specialist client-side PM be brought in?
A: Ideally, right at the start, at the feasibility or business case stage. That's where we have the greatest control over risk.
Once you're into construction and the design's done, if it hasn't captured and mitigated your risks, to some extent, it's too late.
The earlier you get in, the earlier you identify the risks, and the more you can mitigate or minimize them as you move through the project phases.
Q: How do you actually surface those risks and then design them out?
A: Risk is a main focus of almost every meeting, whether that's design, client, user group, or construction. There's a risk item on every agenda.
We run risk workshops and risk management plans that are constantly reviewed, so it's a live thing.
In the feasibility or business case, we identify the major delivery and design risks and workshop with the client on how we'll manage or completely mitigate them, and at what stage. Sometimes a design risk means bringing in specialist engineers or consultants to develop strategies and solutions.
It comes down to keeping it front of mind, on the agenda every meeting, keeping everybody informed, and coming up with solutions together.
Q: On a live hospital redevelopment, what are the risks that come up again and again?
A: The biggest is keeping the hospital operational, which comes down to power, air conditioning, and medical gases. Accidentally cutting or shutting down a hospital is a significant issue, so it's managed through the design phase as well as construction.
You look at how to stage the works and how the contractor installs and works around having to cut or reduce services.
Infection control is another big one. We mitigate it through design where we can, but a lot of it comes down to construction methodology.
The best approach is complete separation of the work zone from clinical spaces, using drop sheets, plastic, and even temporary insulated panel walls. The design carries it too, and theaters run on separate HEPA-filtered mechanical systems and are designed to be cleaned easily.
That's also why hospitals are so cold. The low temperature helps manage infection, and theaters are colder again, because bacteria and condensation are the enemy.
Humidity control matters in theater spaces, especially.
Q: Any risks that are a bit more left-field but still land on the list?
A: Equipment integration is one we've been working on a lot lately. We've got people on the team who were biomedical engineers before they became project managers, with backgrounds in asset management in large tier-one hospitals.
They understand the clinical language, can convey design and construction issues to clinicians, and take operational and infection-control issues back to designers.
Integrating major medical equipment such as MRI (Magnetic Resonance Imaging) machines, cath labs (catheterization laboratory), and theater equipment means coordinating with ICT (Information and Communications Technology) systems, building systems, and backup power. You have to make sure all the infrastructure is in before the equipment is rolled in, so it can be turned on and operational from day one with little to no risk of failure.
You don't want someone lying on the theater bed and the equipment failing because of an integration issue. There's not much redundancy you can build in, so knowing how to commission it and what questions to ask is the key.
Equipment Procurement, Design Review, and Health Facility Guidelines
Long-lead equipment and the Australian Health Facility Guidelines shape these projects before a contractor is ever appointed. Here's how procurement and design decisions get made, and how the client signs off.
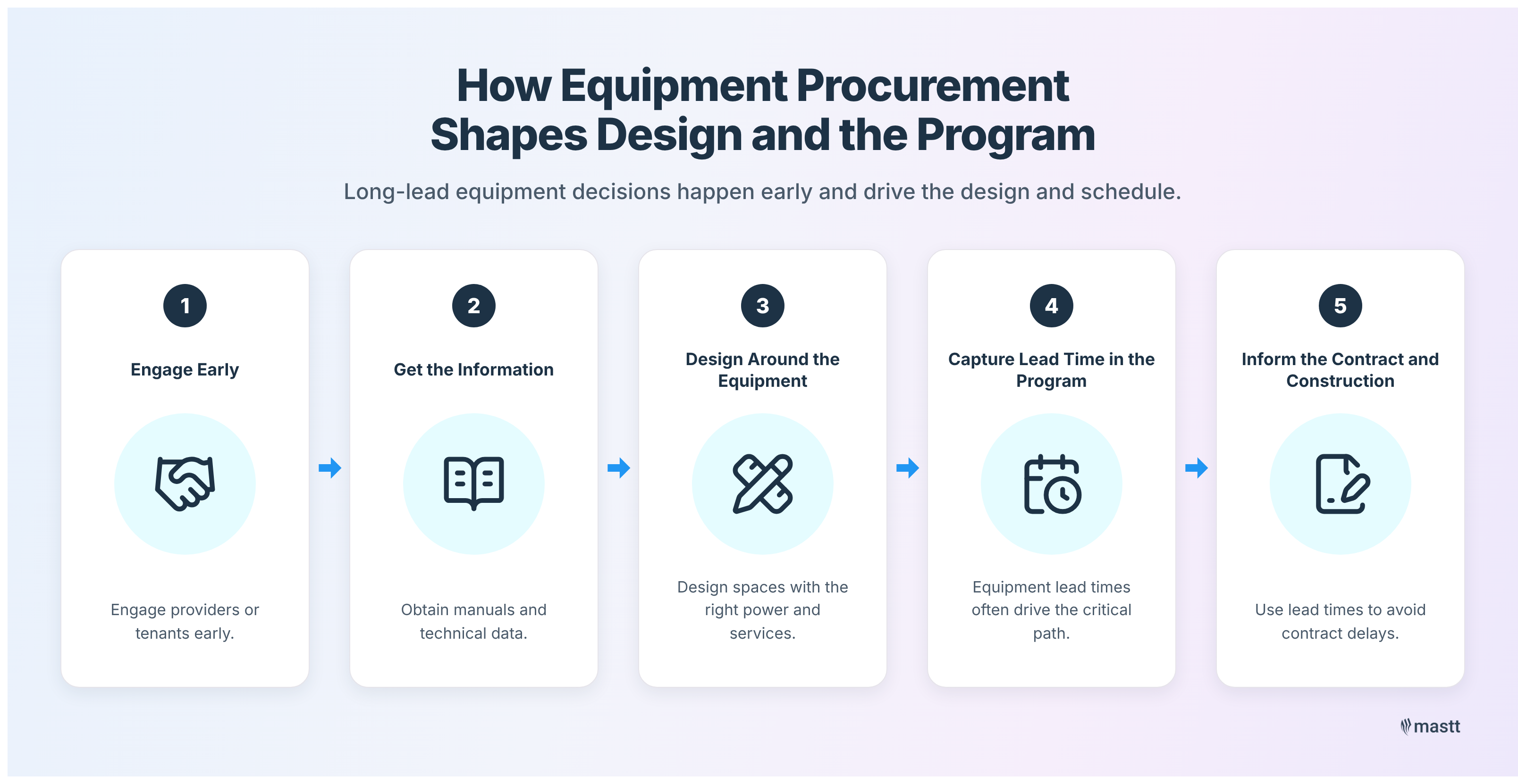
Q: These are long-lead, high-value pieces of kit. How does procurement shape the design and the program?
A: It's done very early. For a medical imaging space with CTs (Computed Tomography) and MRIs, you need to know whether a tenant, say a Queensland X-Ray, is procuring their own equipment through their own supply agreements, or whether it's a Queensland Health-managed facility procuring it.
Either way, you engage those people as early as possible to understand the models, get the operation and maintenance manuals and design information, and design the spaces around them, with power in the right place and building services sized correctly and located properly. Then you have to understand the lead time and capture it in a detailed master program, because in a lot of cases, that drives the critical path.
At the construction contract stage, that matters, so you're not delaying a contractor unnecessarily and costing the client delay damages.
The first step is always the purpose of the facility. You're designing a box around the intended use, whether that's beds with oxygen and nitrous on the wall, a medical imaging unit, a CSSD, or a theater.
Q: You mention the Australian Health Facility Guidelines. How do they sit alongside the building code?
A: The National Construction Code is the legislative requirement. The Health Facility Guidelines are guidelines used as a starting point to design health spaces.
They cover reception and triage areas, waiting rooms, wards, storerooms, and cleaners' rooms.
New greenfield sites mostly comply, but every theater might do different types of operations, so a space might need to be larger, or there might be a good case to make it smaller. You can depart from the guidelines, but it's good practice to identify the departures and document good reasons for them.
Q: Faced with a huge stack of drawings, the code, and the guidelines, how does the PM add value and make sure the design is fit for purpose?
A: We do our own review using our experience, but we also coordinate review sessions with the client and bring in the consultants to present their design. You get a room of stakeholders collectively reviewing, asking questions, and challenging the design, giving everyone comfort that what's been produced is correct and can proceed.
Project managers aren't clinicians. We know enough to be dangerous, but we're not certifying anything, so the end user has to understand and accept the design.
Best case, and it doesn't always happen, we get clients to put a physical signature on each design drawing. That's best practice in my experience, because it means they take responsibility for reviewing and understanding it.
We bring them on a journey through concept, schematic, detailed design, and construction-issue drawings, with user group meetings for the people who'll use specific spaces. At the end of each phase, there's a review, either a desktop review or, ideally, a workshop where we do a page turn.
Their comments are captured and integrated into the next phase, or we come back with reasons they can't be. We'll go through electrical and mechanical drawings too, though usually not the technical detail.
What matters is where the lights are in a theater, the temperature range, the humidity control, and the interfaces they'll use day to day.
“The worst thing that can happen is a client skips through a design, doesn't ask questions, it gets into construction, and then it's not what they're expecting.”
- Gordon Grover
Contract Strategy and Client Setup on Health Projects
Who sits on the client side varies enormously, and so does how a hospital makes money. Both shape how Gordon structures a contract and hands over the design.

Q: Who is on the client side coordinating all those people?
A: It's different for every client. Sometimes there are multiple stakeholders and relationships we have to manage.
Other times, there's one key person, a project sponsor or project manager, that we deal with day to day, and they corral their own stakeholders.
Even within one client, there can be different departments with different levels of interest. The more sophisticated clients, like St Vincent's, usually have one key contact who works in the background, pulling information out of the business.
Others might only do a new capital project once every thirty years, and they don't have that capability, so we do a lot more stakeholder management and education through the whole process.
Q: Hospitals are businesses. How much do their commercials affect your role?
A: In the private space, definitely. Public hospitals have budgets and a set amount of funding for operations and capital works (capital projects), but it's not a profit exercise, and a lot of private hospitals are not-for-profits too.
In the private space, it's all about theaters, running them flat out, as many operations as possible, because that's where a large portion of the revenue comes from. Having to shut a theater down for a refurbishment is a big issue, and when we refurbish a CSSD, shutting it down shuts the theaters too, so keeping it operational throughout is incredibly important.
I run the construction budgets, not the hospital P&L (Profit & Loss), but I do know the private space is struggling. Private health insurance isn't providing the income it used to, and a lot of operators are battling to break even.
It's hard to maintain and upgrade facilities when you're not making the money to set aside for it.
Q: When should the design be handed to the contractor, early or fully documented?
A: It depends on the facility. We go back to what the risks are and who's best placed to manage them, the client or the contractor.
A simple medical ward is an obvious case for design and construct, where you might produce a 30 or 40% design and hand it over for the contractor to finish.
But hand over a 30 or 40% design for a CSSD or an ICU, and you lose a lot of control in the final stages of design. Those are the cases where you progress to 80, 90%, or even fully documented, to keep control of the end product.
Call it contract strategy, procurement strategy, or delivery strategy. It's really about identifying the risks and setting the contract up so the risk share is appropriate.
Q: What are the key documents at the end of design, before going to market?
A: For a design and construct contract, there's a principal's project requirements brief, which documents the requirements the principal wants in their facility that may not already be in the design.
There's a preliminary specification covering what the contractor has to do and provide during construction, and during design on a D&C. That includes producing design documentation for review at set times, updated programs, monthly reports, site facilities, and sometimes an office or meeting room for the client.
Then there's the contract itself in draft form, so they understand their obligations if awarded, plus tender conditions and tender forms for pricing, methodology, and proposed subcontractors.

Q: Does procurement of the major equipment sit with the contractor or the client?
A: Usually, the client or the tenant procures the major equipment, mostly because of the long lead times. You have to place orders well before a contractor is even on board.
We'll write obligations into the contract, so the contractor might be responsible for getting the infrastructure and power in the right location, or for skating in and positioning a large piece of equipment. But the purchase itself is the client's, sometimes assisted by a consultant or by us.
Responsibility almost always stays with the client. If it's ready early, it's stored off-site until the space is ready, and a lot of this equipment is installed, commissioned, and tested right at the death of construction or in an operational commissioning period after practical completion.
We manage it through what we call the FF&E schedule, which sets out who's responsible for procuring and installing each item. We might pass fixed equipment to the contractor to supply and install, but loose or major medical equipment almost always stays with the client.
They're builders, not biomedical engineers, and they're not going to manage a team building an MRI machine.
Assessing Tenders on Complex Health Construction Projects
In government work, the tender process is tightly governed. Gordon explains how he weighs price against experience, and where the best contractor ideas come from.
Q: For complex health work, how do you assess tenders?
A: On government facilities, you comply with the procurement policy. In Queensland, that means assessing the non-price elements before you even look at price.
With the client, we set criteria and weightings based on the risk, so for a highly complex, high-risk project, the non-price criteria significantly outweigh price. Experience having done it before, similar facilities delivered, and a demonstrated understanding of the project and its risks are the key pieces.
Q: Are contractors getting more innovative in how they bid?
A: Yes. A good example is a CSSD refurbishment we did for St Vincent's, ten-plus stages, managing infection control while maintaining operations.
Some genuinely innovative methodologies came out of it, including using sandwich panel walls instead of stud and plasterboard.
The panels could be lifted and moved quickly to separate clinical spaces from work zones and keep operations going, and a metallic sandwich panel wall wipes down far more easily than painted plasterboard, so it helps maintain infection control afterward, too.
It wasn't something we'd seen before, and we've brought it into other projects since. It's a good solution for construction staging and for ongoing operations.
What a Client-Side PM Catches on Site During Construction
Complex health jobs need more site presence than their dollar value suggests. Gordon shares what his team catches and why small details carry outsized risk.
Q: What does your involvement look like during construction?
A: It's definitely more than once a fortnight on the high-risk ones. CSSDs aren't big projects.
Some run from two to eight million dollars, not fifty or a hundred or two hundred million.
On any other project at that scale, you'd be on site once a fortnight, but on a CSSD, a theater, or a medical imaging facility, a lot can go wrong, so our team is out several times a week, particularly during high-risk periods of construction.
Q: Have you been on-site and caught something major?
A: We've been on site when a contractor cut through a wall and hit a water pipe, releasing a heap of water into the clinical spaces below, which creates a whole range of issues. We're always picking things up, like ductwork sitting too low in a ceiling void, or dead legs in plumbing.
A dead leg is a length of pipe with no outlet at the end. In a normal project, especially a refurbishment, you'd cut off an outlet and just cap it and leave it.
In a hospital that creates a Legionella risk, you can't leave dead legs. You have to bring the pipework all the way back.
It's the same logic as the vinyl floors, because carpet in a ward could be stained with blood, feces, or urine, so floors have to be cleanable. Almost everything traces back to infection control.
A Contrarian View on Fully Documented Construction Design
After nearly twenty years, Gordon holds one strong opinion about how the industry documents and delivers design, and why it has slipped.
Q: After nearly twenty years, do you hold a contrarian view you feel strongly about?
A: There's no such thing as a perfect project. There's always something unexpected.
But I've always held out hope that a client would let us run a project the way we think it should be run, and in nearly twenty years, it's never happened.
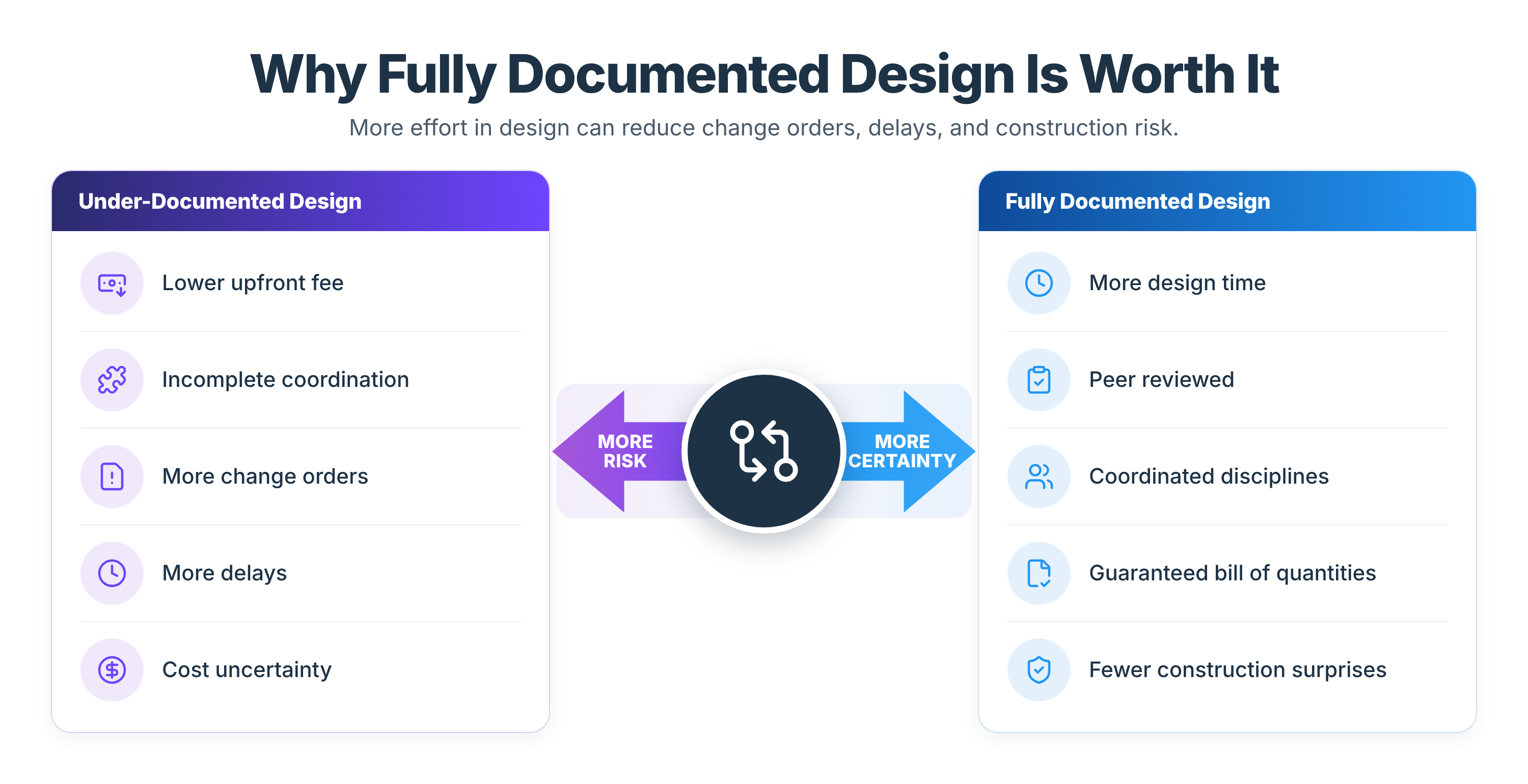
The best way would be to appoint the best consultant in each discipline rather than a large multidisciplinary firm where you get a good mechanical engineer, an average electrical engineer, and a terrible hydraulic engineer. Then run a genuinely fully documented design that is peer-reviewed and coordinated across every engineering discipline and the architect.
I don't mean today's level, where you get a million variations and the delays that come with them. I mean documentation detailed enough that it might take 50% more time to produce, ending in a guaranteed bill of quantities for the contractor to build from.
That's very rarely done today. It costs substantially more in the design phase, but it saves time for the builder and minimizes the risk and cost of variations during construction.
“It will cost substantially more in the design phase. But the saving is in time to the builder and in minimizing the cost of variations during construction.”
- Gordon Grover
Q: Why has the industry gone backward on this? Wasn't BIM meant to fix it?
A: I think it's competitiveness, a race to the bottom in the consulting world. There should be a far higher weighting on experience and capability than price, but price is always a major factor.
You won't win a work tender by offering a properly fully documented design when someone else is pricing one; they call it fully documented, that's really only 80 or 90%, or copy-and-paste construction details from their last project.
When I started in the industry, I worked on a few projects with guaranteed bills of quantities, and the level of documentation was far superior to what's done today, with very minimal variations. Construction timeframes drop too, because everyone knows what they're building.
It's fully coordinated, with construction details that are actually considered rather than copied and pasted. Spending more time planning and developing the design ultimately results in a better outcome for everybody.
Q: How should clients protect themselves from that?
A: Be wary of having the wool pulled over your eyes. It's hard because clients often aren't sophisticated industry professionals, so it's hard to educate them through a tender and hard to sell them on value when they're just looking at price.
And it comes back to the ROI (Return on Investment) problem. How do you show you've saved a client three months or a million dollars when, because you mitigated the risk up front, it never actually happened?
I've been talking about that for twenty years. I haven't seen anyone do that ROI piece really well, but with enough data, I reckon it's possible.
“How do you demonstrate that you've saved a client three months or a million dollars when it never actually happened?”
- Gordon Grover
How to Deliver Complex Health Construction Projects
Complex health projects reward one thing above all, and that's experience that has met the risk before. Gordon's approach puts risk management at the center from feasibility onward. The harder problem, proving the value of risks prevented before they ever surfaced, is one he is still working on after twenty years.
“We wouldn't have a job if anybody could do it.”
- Gordon Grover
.avif)
Written by
Doug Vincent
Doug Vincent is the co-founder and CEO of Mastt, the AI capital-project management platform used by governments, Fortune 500 companies, and consultancies across APAC, North America, and MENA. Before founding Mastt in 2019, he spent a decade at RPS delivering more than $2 billion in capital works, including the $2.1B Defence Navy Infrastructure program, and holds a CPSPM certification with the AIPM. He contributes content and speaks on AI in capital project delivery at Mastt.


Contributions by
Gordon Grover
Gordon Grover is Managing Director of Specialised Property Consulting, a Toowoomba-based firm delivering project, development, and superintendency services across Queensland. A QBCC-licensed Builder Project Manager, he has delivered projects from $20 million regional health clinics to the $235 million InterLinkSQ freight terminal, and founded the health-infrastructure advisory Specialised Health Advisory. He contributes content on capital planning and project delivery at Mastt.
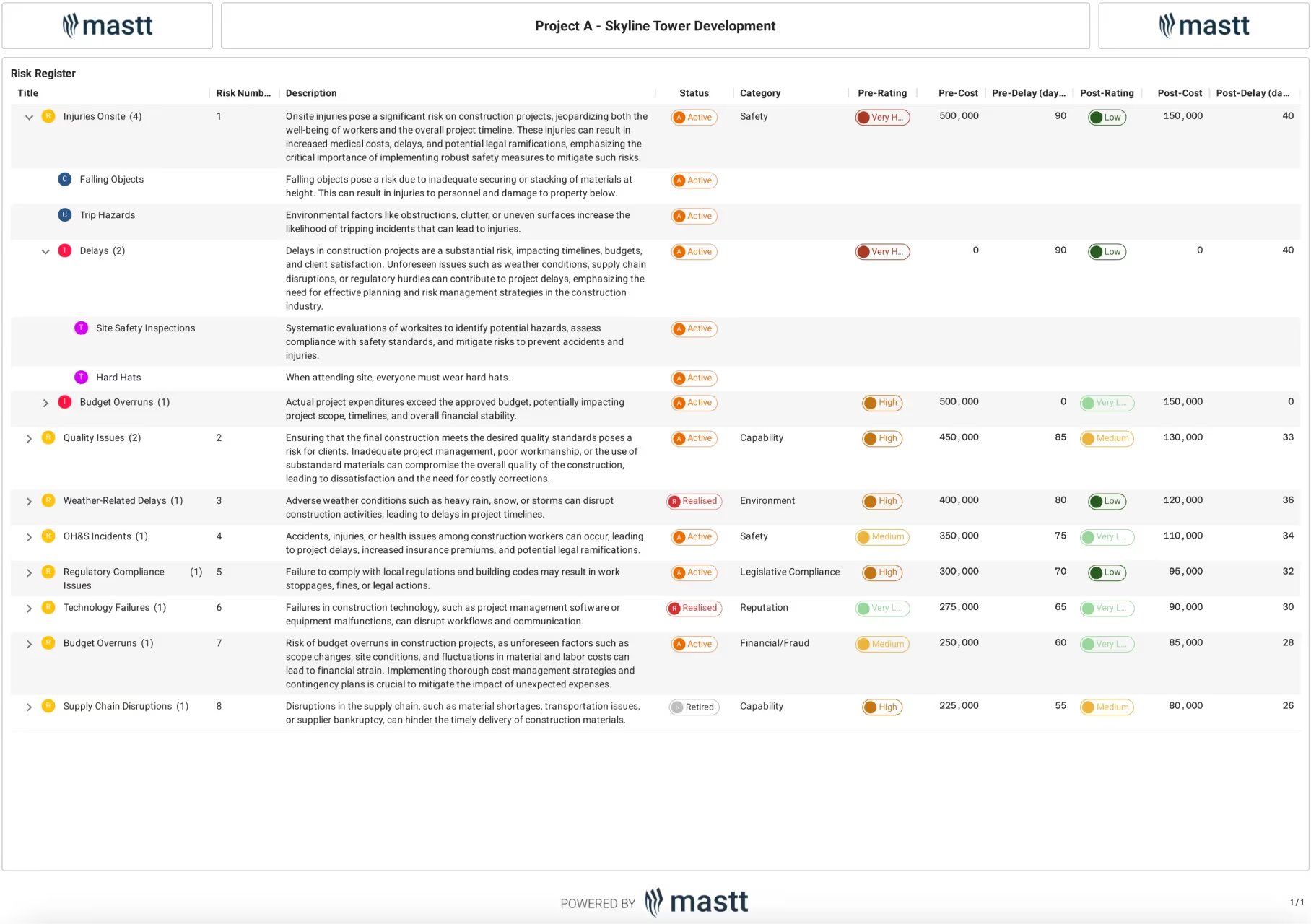
Risk Register Template
Use this FREE Risk Register Template to identify, assess, and treat risks before they escalate. Reduce delays, track cost impacts, and stay compliant using a proven risk format.

Walk Into Every Meeting With Confidence, Clarity, and Control
No one wants to look unprepared, blindsided, or uncertain in front of stakeholders — but that’s exactly what happens without Mastt.
Start for FreeTrusted by the bold, the brave, and the brilliant across governments, Fortune 500s, and the world’s best in delivering the future